ERCP surgery
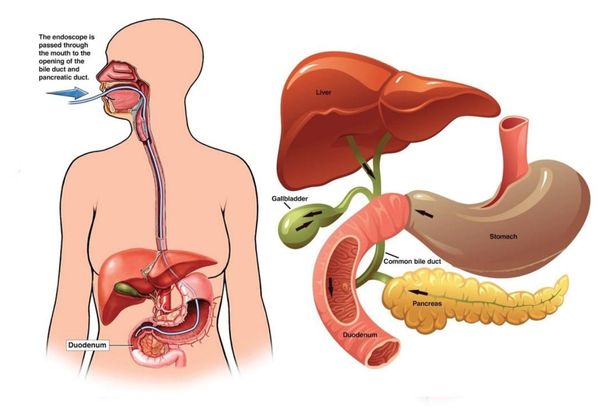
The surgery technique makes use of a combination of luminal endoscopy compiled with fluoroscopic technique of imaging for the purpose of diagnosing and performs treatment of conditions that are associated with pancreatobiliary system. A side viewing instrument named the duodenoscope is utilized in the endoscopic portion that is made to travel through the esophagus and reach the stomach to access the duodenum’s second portion which is the part of small intestine.
In ERCP Sphincterotomy both fluoroscope and endoscope are employed and deep cannulation is done of the bile duct which is then followed by the sphincter of Oddi’s severance with electrocautery (heating).
Coming back to conventional ERCP, next the duodenal pailla is identified with the scope in the position discussed above and further inspection is carried out to find any abnormalities. The duodenal papilla is like a structural protrusion of the ampulla of Vater or the hepatopancreatic ampulla into the duodenal lumen. The ventral pancreatic duct and the common bile duct have a convergence point and that is this ampulla. So this ampulla behaves like a channel for draining pancreatic secretions and bile into the duodenum.
If contrast is injected into the pancreatic duct or if the pancreatic duct gets cannulated for quite a number of times then a temporary pancreatic duct stent placement or rectally administered NSAIDS (diclofenac or indomethacin) has to be considered. This has to be considered aiming to reduce the post-ERCP pancreatitis (PEP) risks. For PEP prophylaxis these two prevention modalities have shown some promise. Somatostatin, gabexate, heparin, nitroglycerin, allopurinol, steroids, octreotide and many more pharmacological agents have been studied but the results found were pretty disheartening.
In the second portion or segment of the duodenum the minor duodenal papilla is also located and it behaves like an access point for the dorsal pancreatic duct. Dorsal pancreatic duct’s evaluation with ERCP is seldom performed and the ERCP indications are further discussed below:
With the side viewing endoscope the papilla is closely examined and then selective cannulation of ventral pancreatic duct or common bile duct is performed. Once the cannulation of the selected duct is performed then either pancreatogram of the pancreatic duct or cholngiogram of common bile duct is obtained fluoroscopically with the injection of a material that is radiopaque contrasting in nature is done into the duct. These days ERCP is considered by surgeons like a therapeutic surgery where abnormalities that are observed via a fluoroscope can be particularly addressed by the methods of specialized accessories that can be passed via the endoscope’s working channel.
This procedure is a very advanced process and as a result of this serious complications tend to occur at a higher frequency than many other endoscopic processes. As per that special training and specialized devices and equipments are employed and for appropriate indications only this procedure is employed.
Indications that have been recorded for biliary diseases are given below:
Assessment of biliary obstruction and its treatment secondary to choledocholithiasis- if ascending cholangitis, worsening pancreatitis or worsening jaundice which are persistent are present then Precholecystectomy ERCP may be indicated.
- With intraoperative cholnagiography or common bile duct exploration without the extraction of stone, treatment of choledocholithiasis is identified during cholcystectomy.
- Bile duct stricture assessment and subsequent treatment- bening and malignat strictures and and congenital abnormalities of the bile duct.
- Postoperative complications
- Postoperative biliary leaks’ treatment and assessment
- Sphincter of Oddi dysfunction of selected patients, their assessment with treatment with little benefit in modified Milwaukee classification type III patients
- For recurrent and acute pancreatitis for which the underlying cause is unknown in patients; their treatment followed after assessment
- Symptomatic strictures associated with chronic pancreatitis; assessment and treatment
- Symptomatic pancreatic duct stones; their treatment after assessment
- Symptomatic duct stones’ assessment and treatment
Pancreatic malignancies can be diagnosed and the indications are:
- Biopsy and brushing of the bile duct
- Pancreatoscopy
- Intraductal ultrasonography
There are also indications for ampullary diseases like
- Assessment of ampullary malignancy
- Ampullary adenomas’ assessment and treatment
If a patient has the possibilities of developing post ERCP pancreatitis, then the process of diagnosis grows apparent within some hours after the procedure. The patient shall experience severe pain in abdomen back pain and nauseated feelings may be accompanied with vomiting sensation) and some amount of fever is also common. But then the observation period does not stretch beyond an hour after the ERCP procedure and is not enough time for checking for post ERCP Pancreatitis. For evolving post ERCP pancreatitis a two hour serum or urinary amylase level (>1000IU/L) is highly predictive if the patient can be kept under observation for a longer duration of time.
Another kind of procedure closely related to ERCP is the employment of miniature endoscopes that can be inserted via the operating channel of the duodenoscope. These can be directly inserted into the pancreatic or the bile duct. The interior side of the duct can be visualized and accordingly biopsies can be taken. There remain other possibilities for therapeutic interventions.
If in the common bile duct the bile duct stones are seen then the opening of the papilla will be made wider with the help of electrocautery or heating and then the stones are removed. For removal of stones sometimes a basket may be employed. If the narrowing of the bile duct is seen in the X-ray images then a small wire mesh or plastic tube which is a stent can be inserted to facilitate the bypassing of the blockage and allow the bile to move to the duodenum. Very mild pain after ERCP stent placement is felt.
ERCP Complications
ERCP complication chances are vastly reduced when performed by expert surgeons but still there persists some amount of complications like:
- Pancreatitis or inflammation of the pancreas is the commonly occurring complication found in 3 to 5% of the patients undergoing the surgery. Usually it is mild causing nausea and pain in the abdomen region which can be treated during the stay in hospital. It is very rare that pancreatitis grows severe during ERCP.
- A cut into the ampulla becomes necessary by the endoscopist and as soon as that happen some amount of bleeding can occur at the site of the cut ampulla. However it is minimal and stops in sometime all by itself or it can be controlled during the surgery.
- A tear or hole in the intestine can happen accidentally due to the insertion of the scope or any other instrument. This happens rarely but when it occurs it is a serious condition requiring immediate surgical intervention.
- Infection or cholangitis is also very rare in the bile ducts but if it occurs among patients with preexisting conditions then treatment has to be started where antibiotics need to be administered and drainage of excess fluids need to be carried out.
If by accident food or fluid is inhaled in the lungs then that can be a complication but it rarely occurs in patients who do not drink and eat several hours prior before the ERCP test.